S44
Optimization of Variable TI 4D ultrashort TE MR Angiography: A Numerical Simulation and Phantom Study1Department of Radiology, Juntendo University Hospital, Tokyo, Japan, 2Department of Radiology, Graduate School of Medicine, University of Tokyo, Tokyo, Japan, 3Department of Radiology, Juntendo University Graduate School of Medicine, Tokyo, Japan, 4Department of Radiology, Toranomon Hospital, Tokyo, Japan
Synopsis
We implemented the new Variable TI method to multi-phase ASL 4D UTE-MRA in order to improve the visibility of hemodynamic flow. We performed a numerical simulation and a phantom study to find the optimized condition. It was found that a 50 % reduction of TI steps increases 50 % of signal from the flow volume without impairment of structural information.
Background
Arterial Spin Labeling (ASL) based 4D MR angiography (MRA) is commonly applied to assess cerebrovascular diseases. Utilizing multiple ultrashort TE (UTE) enables a suppressed effect on phase dispersion and reduced magnetic susceptibility artifacts1. Compared to digital subtraction angiography (DSA), Variable TI (VTI) 4D UTE-MRA has advantages in the non-contrast agent technique. However, it is beyond the ability of hemodynamic visibility especially in late phases. The signal from arterial blood reduces because of transit-time signal decay. Arterial imaging is important for a range of clinical applications such as follow-up after stents or coil embolization for intracranial aneurysms, endovascular embolization of cerebral arteriovenous malformations (AVM) and dural arteriovenous fistulas (dAVF)2,3. Increasing the number of TI steps brings shorter TI intervals, which leads the longitudinal magnetization into the steady state. As a results, blood signal decays in late phases. As the TI intervals are constant in Conventional 4D UTE-MRA, there is a tradeoff between signal decays and short TI intervals which is needed in the early TI phase. We reported the ability of VTI 4D UTE-MRA in ISMRM2020. It was reported that the hemodynamic in late phases had been improved as an initial experimental study. To keep the temporal resolution in early phases, we adopted TI intervals with a manner of progression of difference. In this study, we optimized TI intervals and the number of TI steps to improve the image quality of the hemodynamic flow in longer TI intervals.Methods
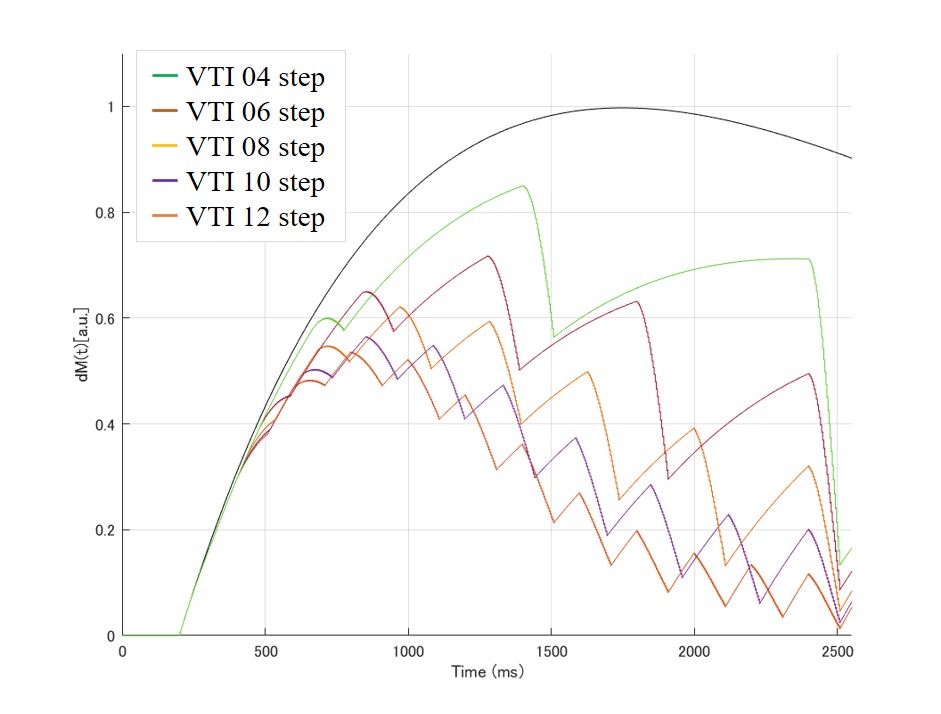
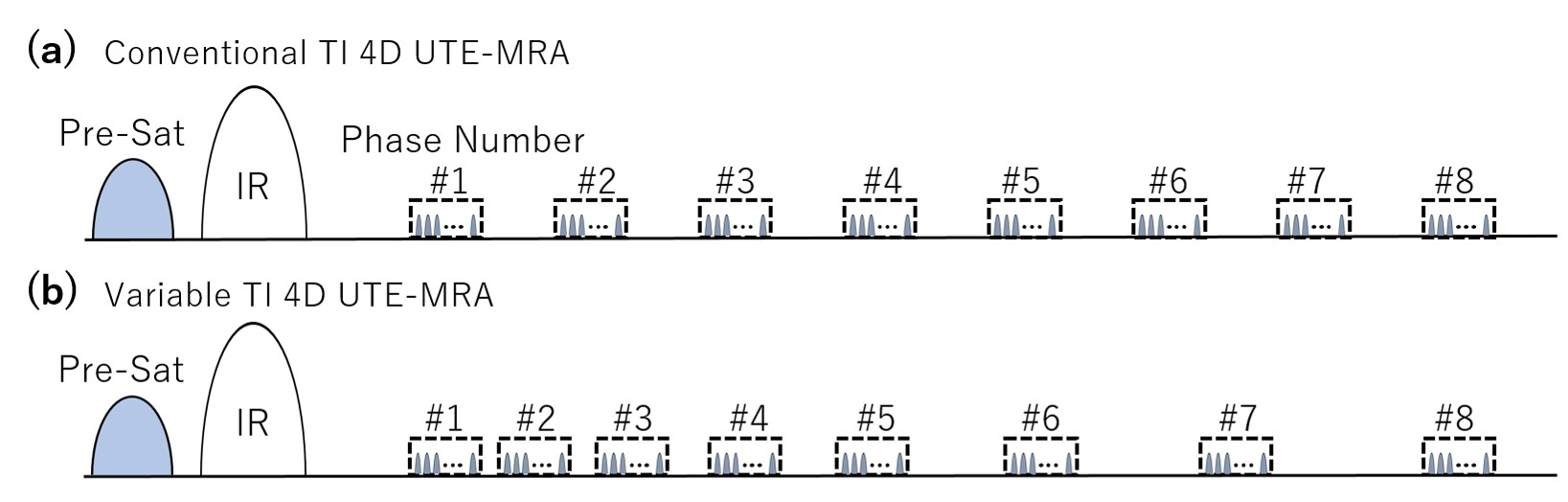
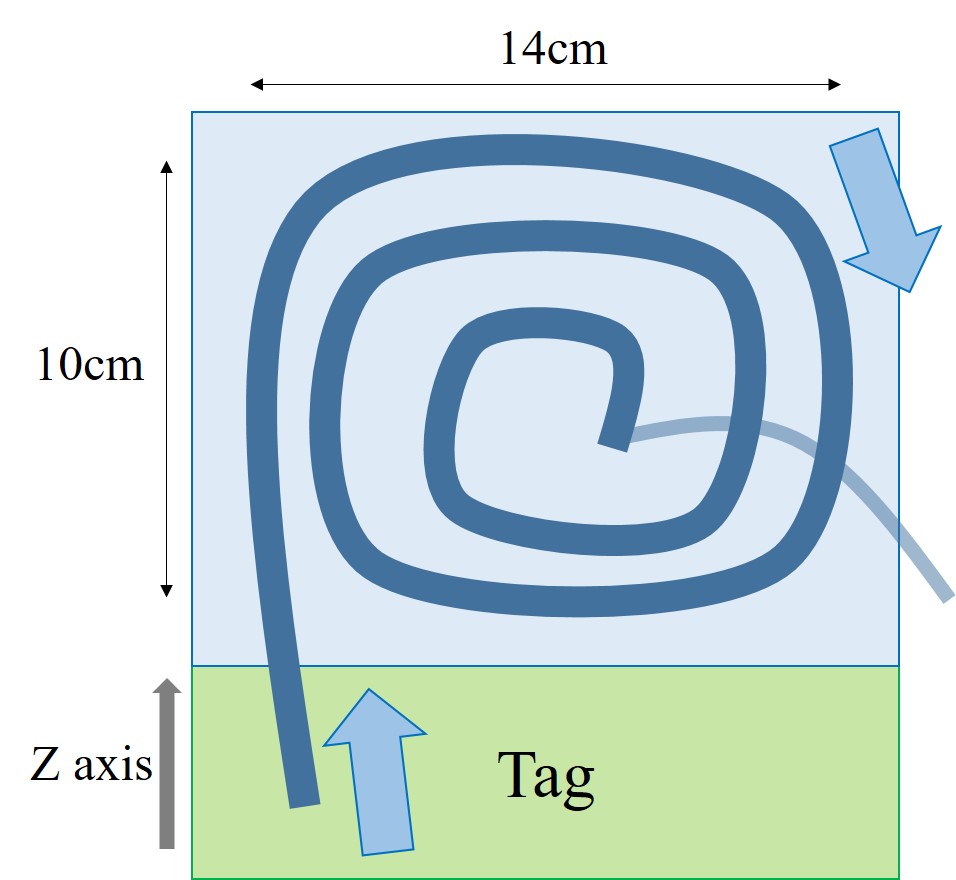
The numerical simulations for blood signal intensity were performed with MatLab (R2019b, MathWorks, Natick, MA). The signal intensity in each phase was simulated by changing the TI intervals and the number of TI steps. We set the first TI step to 200 ms and the last TI step to 2400 ms in both the conventional and the VTI method (Figure.1).The flow phantom study was performed with original spiral tubular phantom simulating a cerebral blood flow with 4 mm inner diameter of silicon tube with a pulsatile flow rate of 60 pulses per minute with 30 to 33 cm/s mean flow velocity (Alpha Flow EC-1/Pulsating Flow Water Phantom HB-1, FYC Fuyo Corporation, Japan). T1 relaxation time of the flow agent was adjusted to 1850 ms which is equivalent to T1 value of blood at 3 Tesla (Figure.2,3). All subjects were scanned on a 3 Tesla MRI scanner (Vantage Galan 3.0T/ ZGO, Canon Medical Systems Corporation, Japan) using a 32-channel head coil for signal reception. Imaging parameters of Conventional 4D UTE-MRA and VTI 4D UTE-MRA were as follows: FOV = 224 × 224 mm2, acquisition resolution = 1 × 1 × 1 mm3, TR/TE = 3.7/0.1 ms, flip angle = 1.8 to 6 deg, shot interval = 3600 ms, Number of Trajectories = 7950, K-space fill ratio = 5.0 %, scan time = 18 min, start/end TI = 200/2400 ms. In Variable TI, we set each TI steps as follow.
$$TI(last) = TI(start) + TI(step)×(n-1) + TI(delta)×n(n-1)/2$$
where n is the number of TI steps. The Conventional 4D UTE-MRA of 12 steps utilize equally time intervals between each TI. The mean of region of interest (ROI) were measured at the similar location from the source image.
Results
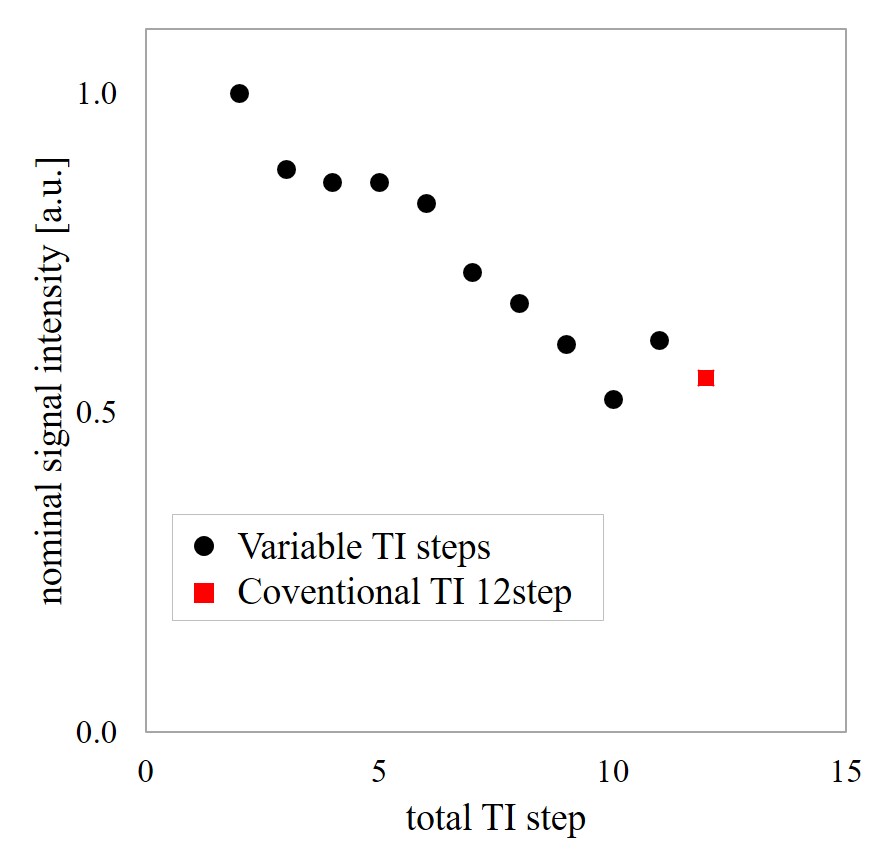
As shown in Figure 4, the coronal of maximum intensity projection (MIP) of all TI steps addition image were displayed to evaluate the continuous blood flow dynamics. The overall signal intensity in the tube improved as the number of TI steps were decreased. When the number of TI steps were 2 to 5 steps, continuous blood flow dynamics in the tube could not be evaluated due to the long shot intervals.Figure.5 showed the mean of ROI of the similar location of the last TI in the source image. The signal intensity under the condition of 6 acquisitions of VTI step was 50 % higher than that of the Conventional TI step method using 12 acquisitions. Both MIP and the mean of ROI of VTI 4D UTE-MRA at the last TI improved the depiction ability compared to Conventional 4D UTE-MRA. In particular, the visibility of the blood flow at late phase was the best when the number of TI steps was 6.
Conclusions
In conclusion, we found the optimum imaging conditions for VTI 4D UTE-MRA in a phantom study. When the number of TI steps was 6, it was revealed that the 50 % of reduction of TI steps increase 50 % of signal from the flow volume without impairment of structural information.Acknowledgements
No acknowledgement found.References
1. Irie R, Suzuki M, Yamamoto M, et al. Assessing Blood Flow in an Intracranial Stent: A Feasibility Study of MR Angiography Using a Silent Scan after Stent-Assisted Coil Embolization for Anterior Circulation Aneurysms. AJNR Am J Neuroradiol. 2015: 36(5): 967-970.
2. Kang J H, Yun T J, Rhim J K, et al. Arterial spin labeling MR imaging aids to identify cortical venous drainage of dural arteriovenous fistulas. Medicine (Baltimore). 2018: 97(19): e069.
3. Choi J W, Roh H G, moon W J, et al. Time-resolved 3D contrast-enhanced MRA on 3.0T: a non-invasive follow-up technique after stent-assisted coil embolization of the intracranial aneurysm. Korean J Radiol. 2011: 12(6): 662-670.
Figures