3363
Phantom Experiments for Optimal Soft Gating Parameter in Free-Breathing Hepatobiliary Phase MRI with KWIC Reconstruction
Tomohiro Noda1, Keitaro Sofue2, Ryuji Shimada1, Yuichiro Somiya1, Shintaro Horii1, Yoshiko Ueno2, Naoki Yoshida1, Yu Ueda3, Akiko Kusaka1, and Takamichi Murakami2
1Center of Radiology and Radiation Oncology, Kobe University Hospital, Kobe, Japan, 2Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 3Philips Japan MR Clinical Science, Tokyo, Japan
1Center of Radiology and Radiation Oncology, Kobe University Hospital, Kobe, Japan, 2Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 3Philips Japan MR Clinical Science, Tokyo, Japan
Synopsis
In free-breathing radial k-space sampling with KWIC reconstruction, soft gating method can be adopted to reduce motion artifacts. We investigated optimal soft gating parameters for free-breathing hepatobiliary phase MRI. A programmable respiratory motion phantom with varying motion distance of 10, 20, 30 mm was imaged using six values of soft gating factor (SGF). Image contrast and sharpness were analyzed by calculating contrast ratio (CR) and full width at half maximum (FWHM). The CR and FWHM were not inferior compared with the reference standard images in any of the motion distances when the SGF was set at more than 1.4.
Introduction
Hepatobiliary phase imaging achieves exceptional contrast enhancement of liver parenchyma, which enables excellent detection of focal liver lesions in gadoxetic acid-enhanced MRI. Radial k-space sampling with k-space weighted image contrast (KWIC) reconstruction is a useful tool for obtaining imaging data under free-breathing and has been clinically applied in patients with impaired breath-holding capability (1, 2). In free-breathing protocol, soft gating method has been proposed to reduce motion artifacts with keeping image contrast by reconstruction of motion-weighted data based on a navigator signal (3). Although oversample factor in respiratory soft gating can be modified according to the roughness of the respiration in free-breathing radial gradient echo sequence with KWIC reconstruction (Figure 1), the effect of the oversample factor on image quality has not been fully investigated. The purpose of this study was to investigate optimal soft gating parameters for free-breathing hepatobiliary phase MRI with KWIC reconstruction using respiratory motion phantom.Methods
A commercially available programmable respiratory motion phantom (QUASAR™ MRI4D Motion Phantom, MODUS QA, Canada) was filled with gadoxetic acid diluted saline solution (T1 value = 245 ms) to simulate the background liver parenchyma on hepatobiliary phase image. Saline-filled sphere 20 mm in diameter simulating focal liver lesion were inserted in the solution. The phantom was commanded to make a piston movement for 12 times/min. simulating respiratory motion, and the motion distance was set at 10, 20, and 30 mm by using a software (Respiratory Motion QA, MODUS QA). The phantom was imaged using a radial gradient echo sequence with KWIC reconstruction (4D FreeBreathing, Philips) at a 3.0T MR scanner (Ingenia 3.0, Philips Medical Systems). Six values of the soft gating factor (SGF) were set to evaluate the image quality, and radial scan percentage (RSP) was accordingly modified to keep the same acquisition time (Figure 2). For the reference standard images, the phantom was also imaged using maximum values of the SGF of 2.0 and RSP of 235 (Figure 3). Other imaging parameters were set as follows: field of view: 256 x 256 mm, matrix: 256 x 256, TR: 4.2 ms (shortest), TE: 1.67 ms (shortest), flip angle: 15 degree, TFE factor: 29, parallel imaging factor: 1.8, and half scan factor: 0.85. From the obtained images, regions of interests were placed to measure signal intensities (SIs) on the background gadoxetic acid diluted saline solution and saline-filled sphere in the six imaging sets with combinations of the SGF and RSP on ten slice images. Contrast ratio (CR) between the background and lesion was calculated using the following formula:CR = SI of the background – SI of the lesion / SI of the background.
We also calculated full width at half maximum (FWHM) to evaluate the sharpness between the background and lesion by using horizontal distance of the background across maximum diameter of the lesion in an image slice. The CR and FWHM for the six imaging sets were compared with reference standard images by using Mann-Whitney's U test on each motion distance.
Results
The image contrast and sharpness decreased as the motion distance increased (Figure 3). The CR was significantly affected in the imaging set with SGF of 1.025 on the motion distance of 10 mm (P =0.013). In the motion distance of 20 and 30 mm, CRs in the imaging set with SGF of 1.025 and 1.2 were significantly lower than that with the reference standard images (P <0.01) (Figure 4). Regarding the FWHM, no significant differences were observed in the six imaging sets on the motion distance of 10 mm. However, the FWHMs were significantly longer in the imaging set with SGF of 1.025 on the motion distance of 20 mm (P <0.001) and imaging sets with SGF of 1.025 and 1.2 on the motion distance of 30 mm (P <0.001) (Figure 5). In consequence, when the SGF was set at more than 1.4, the CR and FWHM were not inferior compared with the reference standard images in any of the motion distances.Discussion
The soft gating method can achieve motion robustness by incorporating respiratory states into reconstruction of motion-weighted data and has been implemented in free-breathing hepatobiliary phase MRI using radial gradient echo sequence with KWIC reconstruction. In our phantom experiments, the CR and FWHM between the background and lesion were influenced by the parameter of SGF as the motion distance increased. On the other hand, the CR and FWHM were similar to the reference standard images when the SGF was set at 1.4 or higher, which may be because k-space sampling could be obtained from more stable data during expiratory state.Conclusion
Our phantom study suggests that soft gating factor influenced on image contrast and motion artifact in 4D FreeBreathing sequence. For the maintenance of robust and good image quality, the soft gating factor needs to be set at 1.4 or higher regardless of the motion distance in free-breathing hepatobiliary phase MRI using radial sampling with k-space weighted image contrast reconstruction.Acknowledgements
I would like to thank MRI staffs in Center of Radiology and Radiation Oncology for help with data collection and useful discussions.References
- Reiner CS, Neville AM, Nazeer HK, et al. Contrast-enhanced free-breathing 3D T1-weighted gradient-echo sequence for hepatobiliary MRI in patients with breath-holding difficulties. Eur Radiol. 2013; 23(11): 3087-93.
- Yoon JH, Lee JM, Lee US, et al. Navigated three-dimensional T1-weighted gradient-echo sequence for gadoxetic acid liver magnetic resonance imaging in patients with limited breath-holding capacity. Abdom Imaging. 2015; 40(2): 278-88.
- Johnson KM, Block WF, Reeder SB, et al. Improved least squares MR image reconstruction using estimates of k-space data consistency. Magn Reson Med. 2012; 67: 1600-8.
Figures

Figure 1: Schematic drawings of respiratory cycle (a) and soft gating method in radial k-space sampling with KWIC reconstruction (b). In the KWIC reconstruction, central k-space data are obtained from only the current temporal phase. Soft gating factor (SGF) means emphasis degree of the obtaining data in the expiratory state. For example, the SGF of 2.0 refers filling central k-space from a half of the data within the expiratory state during respiratory cycle.

Figure 2: Combination of soft gating facto and radial scan percentage for the phantom experiments.

Figure 3: The reference standard images of the respiratory motion phantom show that image contrast and sharpness decreased as the motion distance increased.

Figure 4: Box plots show the results of CR. Each CR was compared with reference standard images. The CR was significantly affected in the imaging set with SGF of 1.025 on the motion distance of 10 mm. In the motion distance of 20 and 30 mm, CRs in the imaging set with SGF of 1.025 and 1.2 were significantly lower than that with the reference standard images.
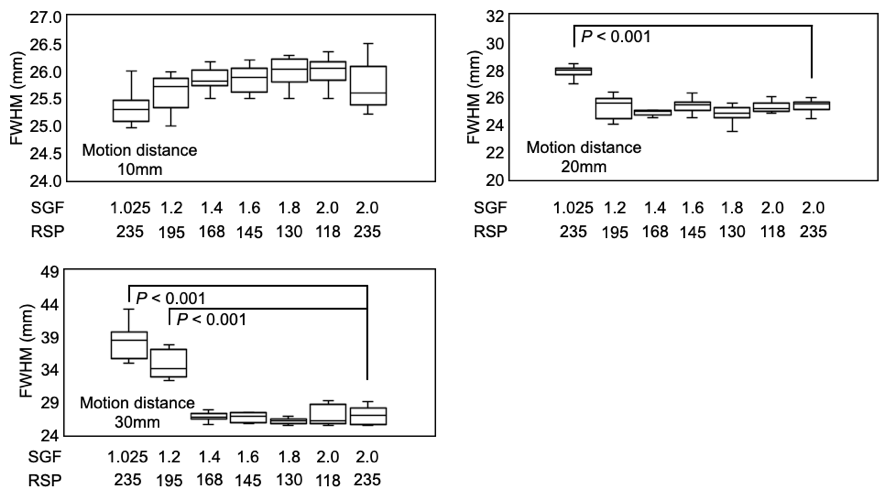
Figure 5: Box plots show the results of FWHM. Each FWHM was compared with reference standard images. There were no significant differences in the six imaging sets on the motion distance of 10 mm. The FWHMs were significantly longer in the imaging set with SGF of 1.025 on the motion distances of 20 and 30 mm.