0706
Volumetric fetal flow imaging with rapid multislice multidimensional radial phase contrast MRI1Medical Biophysics, University of Toronto, Toronto, ON, Canada, 2Translational Medicine, The Hospital for Sick Children, Toronto, ON, Canada, 3Labatt Family Heart Centre, The Hospital for Sick Children, Toronto, ON, Canada, 4Radiology & Nuclear Medicine, Amsterdam University Medical Centers, Amsterdam, Netherlands, 5Pediatric Cardiology, The Hospital for Sick Children, Toronto, ON, Canada, 6Department of Pediatrics, University of Toronto, Toronto, ON, Canada
Synopsis
In this study, we demonstrate multidimensional fetal blood flow visualization and quantification, using highly accelerated multislice radial phase contrast MRI with slice-to-volume reconstruction. This acquisition and analysis pipeline provides real-time reconstructions for in-plane motion correction and cardiac gating for subsequent CINE reconstruction. CINEs are combined into a dynamic flow sensitive volume using slice-to-volume reconstruction with interslice motion correction. Experimental validation is presented in two adult volunteers. Feasibility is demonstrated in four human fetuses capturing complex hemodynamics in the fetal circulation.
Introduction
Fetal development relies on a complex circulatory network that includes physiological shunts such as the ductus venosus, ductus arteriosus, and foramen ovale1,2. Accurately assessing this flow distribution is important for understanding pathologies and potential therapies.In this work, we demonstrate a method for volumetric multidimensional imaging of fetal flow using radial phase contrast (PC) MRI. Fetal application of PCMRI faces several challenges: small vascular structures, high fetal heart rates, uncontrollable motion, and lack of traditional cardiac gating methods. Recent advances in accelerated and motion compensated PCMRI have enabled quantitative assessment of the fetal circulation in which real-time reconstructions are used for intra-slice motion correction and fetal heart rate extraction to reconstruct multidimensional flow CINEs for a single slice3. Moreover, slice-to-volume reconstruction (SVR) techniques have allowed dynamic volumetric imaging of the fetus with MRI recently4,5. Here, we combine CINEs reconstructed from our accelerated multidimensional radial PCMRI acquisitions with inter-slice spatiotemporal coregistration through SVR to generate 4D fetal cardiac flow reconstructions. We refer to this method as ‘radial SVR flow’. Validation is provided in adult volunteers, with feasibility demonstrated in late gestation human fetuses.
Methods
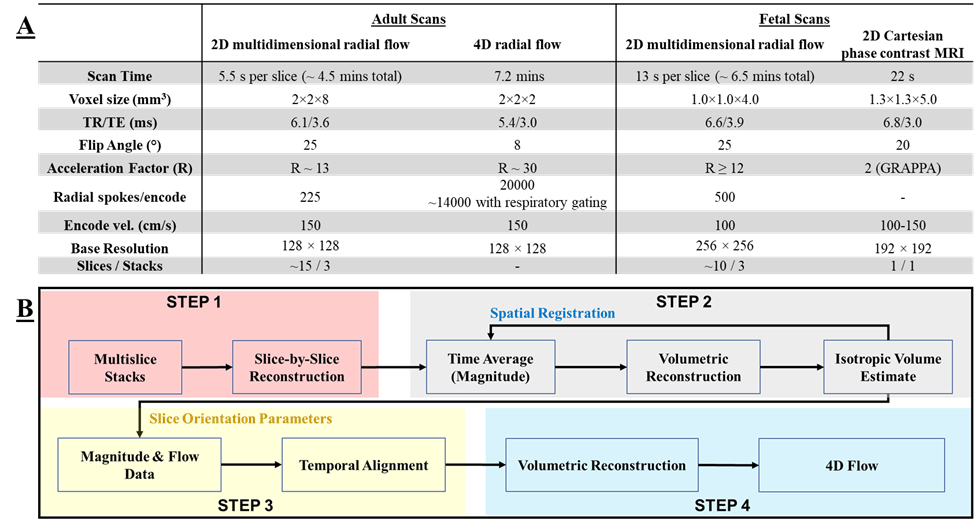
All imaging was performed free breathing on a clinical 3T MRI system (PrismaFIT, Siemens Healthineers) with imaging parameters summarized in Figure 1A. Volumetric flow was visualized using prototype software (4D Flow v2.4, Siemens)6.Validation of the acquisition and reconstruction strategy was performed in two healthy adult volunteers (25 years). Scans were pulse gated and included 3 orthogonal stacks of multislice 2D radial PCMRI with multidimensional flow encoding, used for radial SVR flow reconstruction, followed by a reference 4D PCMRI radial acquisition (3D scan retrospectively binned into cardiac phases)7. Radial SVR flow (Figure 1B) was reconstructed by first reconstructing CINEs for each slice using compressed sensing (CS) followed by SVR. 4D radial PCMRI acquisition was reconstructed using CS.
Feasibility of the approach was tested in four healthy pregnancies (gestational age: 36 ± 1 weeks). Three orthogonal stacks of multislice multidimensional 2D radial PCMRI, centered on the fetal heart, were acquired. Radial SVR flow (Figure 1B) was reconstructed through in-plane motion correction and gating, followed by CINE reconstruction3. CINEs were then combined with SVR. For reference, 2D Cartesian PCMRI acquisitions were performed on the fetal great vessels and reconstructed into CINEs using metric optimized gating8.
Mean flows from the great vessels in the radial SVR flow and reference were compared through linear regression and Bland-Altman analysis.
Results and Discussions
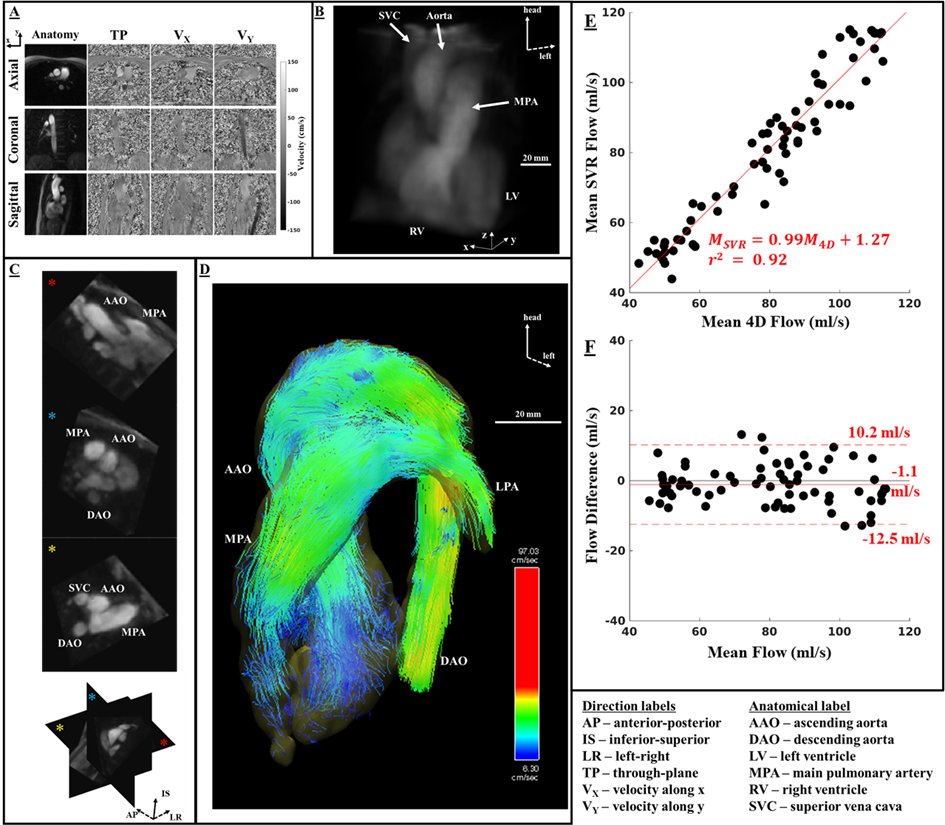
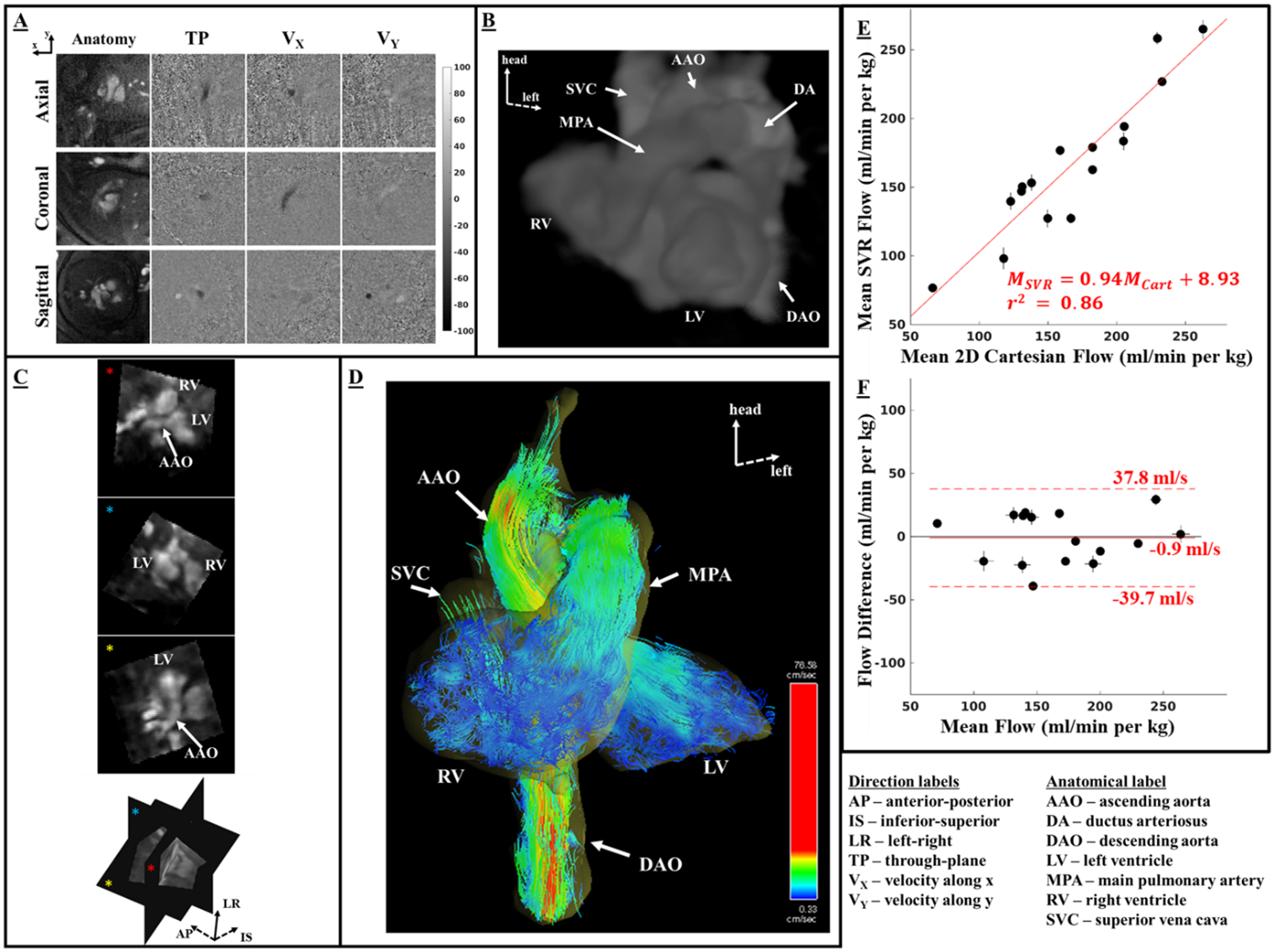
Representative reconstructed CINE frames from one adult subject are presented in Figure 2A. Figure 2B shows a volume rendering of the cardiac anatomy reconstructed with SVR with oblique resampled slices in Figure 2C. Path lines tracking blood flow from start to peak systole are shown in Figure 2D. Comparison of mean flows between the radial SVR flow and 4D radial flow reconstructions is shown in Figure 2E (linear regression: slope = 0.99, intercept = 1.27 ml/s) and 2F (Bland-Altman: bias = -1.1 ml/s, limits of agreement [-12.5, 10.2] ml/s).Representative reconstructed CINEs from one fetus at peak systole are shown in Figure 3A. Figure 3B shows a volume rendering of SVR reconstructed cardiac anatomy with oblique resampled slices in Figure 3C. Figure 3D shows particle traces of blood flow from start to peak systole. Flows measured using radial SVR flow compared well with 2D Cartesian PCMRI (Figure 3E: linear regression with slope = 0.94 and intercept = 8.9 ml/min/kg; Figure 3F: Bland-Altman analysis with bias of -0.9 ml/min/kg and limits of agreement [-39.7, 37.8] ml/min/kg).
Figure 4 and Figure 5 show complex circulatory hemodynamics and preferential blood routes in the fetal heart which corroborate previously demonstrated circulatory physiological mechanisms in animal fetuses9,10. Particle traces depicting flow originating from the distal inferior vena cava (IVC) and ductus venosus (DV) are shown in the Figure 4. While both streams meet in the proximal IVC, the blood streams from the two vessels have limited mixing. Oxygenated blood from the DV preferentially shunts to the left side of the heart and most of the deoxygenated blood from the distal IVC goes to the right side of the heart. Blood that originated from the DV and distal IVC exits the heart through the ascending aorta (AAO) and main pulmonary artery (MPA), respectively. Hence, oxygenated blood from DV feeds the critical fetal organs such as the brain and the heart. Figure 5 depicts particle traces of flow from superior vena cava (SVC) and proximal IVC. SVC blood flows into the right side of the heart while that from the IVC flows into both sides of the heart. Traces in the AAO show that blood originated only from the IVC while those in the MPA show that the blood originated from both the SVC and IVC. Hence, deoxygenated blood from the upper fetal body does not recirculate back to the brain before reoxygenation at the placenta.
Conclusion
We have developed an approach for dynamic volumetric fetal flow imaging using highly accelerated multidimensional radial PCMRI. This enabled visualization and quantification of complex fetal blood flow. This approach may also be useful for studies of complex hemodynamics in uncooperative subjects, such as neonates or the elderly.Acknowledgements
No acknowledgement found.References
1. Rudolph A. Congenital Diseases of the Heart: Clinical-Physiological Considerations. John Wiley & Sons; 2011.
2. Prsa M, Sun L, van Amerom J, et al. Reference ranges of blood flow in the major vessels of the normal human fetal circulation at term by phase-contrast magnetic resonance imaging. Circ Cardiovasc Imaging. 2014;7(4):663-670.
3. Goolaub DS, Roy CW, Schrauben E, et al. Multidimensional fetal flow imaging with cardiovascular magnetic resonance: a feasibility study. Journal of Cardiovascular Magnetic Resonance. 2018;20(1):77.
4. van Amerom JFP, Lloyd DFA, Deprez M, et al. Fetal whole-heart 4D imaging using motion-corrected multi-planar real-time MRI. Magn Reson Med. 2019;82(3):1055-1072.
5. Roberts TA, van Amerom JFP, Uus A, et al. Fetal whole heart blood flow imaging using 4D cine MRI. Nature Communications. 2020;11(1):4992
6. Gulsun MA, Jolly MP, Guehring J, Guetter C, Littmann A, Greiser A, Markl M, Stalder AF. A novel 4D flow tool for comprehensive blood flow analysis. In: Proceedings of the 20th annual meeting ISMRM; Melbourne, Australia; 2012. p. 1176
7. Schrauben EM, Lim JM, Goolaub DS, Marini D, Seed M, Macgowan CK. Motion robust respiratory-resolved 3D radial flow MRI and its application in neonatal congenital heart disease. Magn Reson Med. 2020;83(2):535-548.
8. Jansz MS, Seed M, van Amerom JFP, et al. Metric optimized gating for fetal cardiac MRI. Magn Reson Med. 2010;64(5):1304-1314.
9. Schrauben EM, Saini BS, Darby JRT, et al. Fetal hemodynamics and cardiac streaming assessed by 4D flow cardiovascular magnetic resonance in fetal sheep. Journal of Cardiovascular Magnetic Resonance. 2019;21(1):8
10. Edelstone DI, Rudolph AM. Preferential streaming of ductus venosus blood to the brain and heart in fetal lambs. Am J Physiol. 1979;237(6):H724-729
Figures